 |
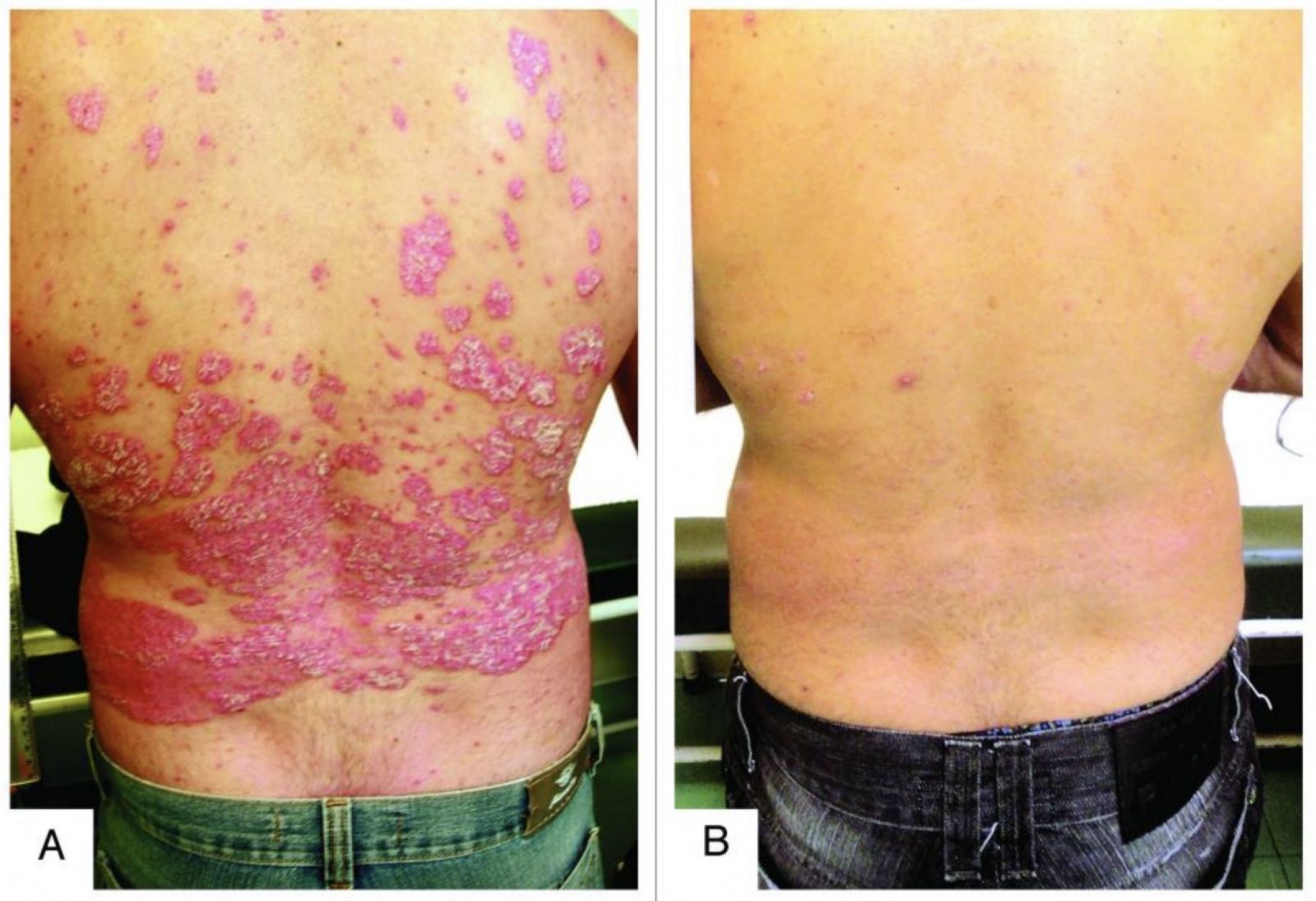
| Dermatoendocrinol. 2013 Jan. C. G. Coibra et. al |
It is now known that multiple mechanisms are involved in the genesis of psoriasis. Those mechanisms are influenced by each individual's genetic predisposition, environment, diet, exercise, body deficiencies, and personality.
Advanced analysis - Metabolomic Analysis® - that detects the metabolic causes of the disease leads to a comprehensive treatment of not just the symptoms but the root causes of psoriasis(10, 15).
Metabolomic Analysis is a Precision Medicine tool that measures tiny molecules that participate in chemical reactions that occur within our cells. It provides accurate data for the personalised treatment and prevention of diseases such as psoriasis and psoriatic arthritis.
Metabolomic Analysis® detects early dysfunctions of the body at the molecular level. It so identifies the different causative factors of psoriasis, which are either inherited (DNA) or environmental (diet, exercise, stress). Metabolomic Analysis accurately measures the organism's deficiencies and malfunctions, helping doctors individualize treatment and prevention approaches.
According to Harvard Magazine and resent research, metabolomics tests are the most accurate method of assessing a person's health. Metabolomics offers a deep understanding of the mechanisms of human health and disease.
Our approach restores the body's normal function. The treatment regimen is tailored to the deficiencies, dysfunctions, imbalances, and needs of the individual patient as they are identified through the Metabolomic Analysis® test. It includes, along with any preexisting symptomatic treatment, the administration of specific supplements, vitamins, trace elements, amino acids, and personalised nutrition.
Through our clinical experience, we have observed that the gradual reparation of these factors results in a steady improvement in the vast majority of cases.
Take the first step today!
Biblioraphic References
”Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics". Menter A, Gottlieb A, Feldman SR, Van Voorhees AS, Leonardi CL, Gordon KB, Lebwohl M, Koo JY, Elmets CA, Korman NJ, Beutner KR, Bhushan R (May 2008). J Am Acad Dermatol.
"Psoriasis". Boehncke, WH; Schön, MP (26 May 2015). Lancet. 386: 983–94. doi:10.1016/S0140-6736(14)61909-7.
Heritability of psoriasis in a large twin sample. Lønnberg AS1, Skov L, Skytthe A, Kyvik KO, Pedersen OB, Thomsen SF. Br J Dermatol. 2013 Aug;169(2):412-6. doi: 10.1111/bjd.12375.
Healthy diet and other lifestyle changes that can improve psoriasis. American Academy of Dermatology.
Integrating lifestyle-focused approaches into psoriasis care: improving patient outcomes? Angelo Landriscina1 and Adam J Friedman. Psoriasis (Auckl). 2016; 6: 1–5. Published online 2016 Jan 19.
An update on psoriasis and metabolic syndrome: A meta-analysis of observational studies. Sanminder Singh, Paulina Young, April W. Armstrong; Published: July 18, 2017. https://doi.org/10.1371/journal.pone.0181039
Psoriasis and insln resistance: a review. Rhea Fitzgerald, Muriel Sadlier, Maureen Connolly and Anne Marie Tobin, Ireland. Christopher T. Ritchlin, M.D., M.P.H., Robert A. Colbert, M.D., Ph.D., and Dafna D. Gladman, M.D. N Engl J Med 2017; 376:957-970March 9, 2017DOI: 10.1056/NEJMra1505557.
A pilot study assessing the effect of prolonged administration of high daily doses of vitamin D on the clinical course of vitiligo and psoriasis Cicero Galli Coimbra et. al. Dermatoendocrinol. 2013 Jan.
Psoriasis, vitamin D and the importance of the cutaneous barrier’s integrity: An update. Carlo Mattozzi, Giovanni Paolino, Antonio Giovanni Richetta, Stefano CalvieriJ Dermatol. 2016 May;43(5):507-14. doi: 10.1111/1346-8138.13305. Epub 2016 Mar 12.
Vitamin D and the Skin: An Update for Dermatologists. Kechichian E1,2, Ezzedine K3,4. Am J Clin Dermatol. 2017 Oct 9. doi: 10.1007/s40257-017-0323-8. PubMED
A pilot study assessing the effect of prolonged administration of high daily doses of vitamin D on the clinical course of vitiligo and psoriasis. Dermatoendocrinol. 2013 Jan. C. G. Coibra et. al.
Association between psoriasis and vitamin D: Duration of disease correlates with decreased vitamin D serum levels. Medicine (Baltimore). 2018 Jun. A. Filoni et. al.
Oral vitamin D, still a viable treatment option for psoriasis. Faranak Kamangar, John Koo, Misha Heller, Eric Lee & Tina Bhutani. Journal of Dermatological Treatment. Volume 24, 2013.
Oral vitamin D3 supplementation for chronic plaque psoriasis: A randomized, double-blind, placebo-controlled trial. Michelle A. Ingram et al. Journal of Dermatological Treatment (2018).
The metabolomics of psoriatic disease Di Yan, Ladan Afifi, Caleb Jeon, Megha Trivedi, Hsin Wen Chang, Kristina Lee, and Wilson Liao. Psoriasis (Auckl). 2017; 7: 1–15. Published online 2017 Jan 31.
 Koumbari 5
Koumbari 5 +30 2103611054
+30 2103611054 info@metabolomicmedicine.com
info@metabolomicmedicine.com